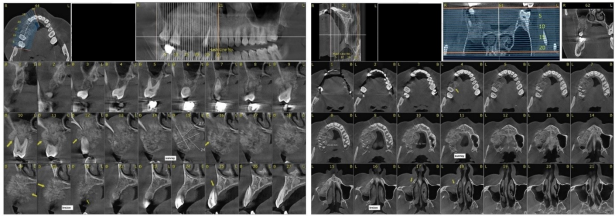
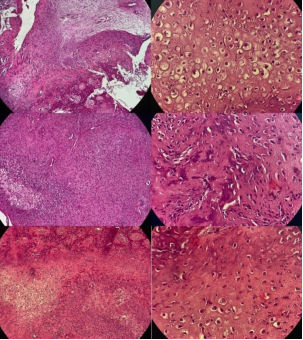
Osteosarcoma is a malignancy of mesenchymal cells that have the ability to produce osteoid or immature bone. Chondroblastic osteosarcoma as constitute a substantial proportion of all osteosarcomas of the jaws. Some examples may be composed almost entirely of malignant cartilage growing in lobules with only small foci of direct osteoid production by tumor cells being identified. Chondroblastic osteosarcoma is a rare and aggressive type of bone cancer that tends to occur in the long bones of the arms and legs, although it can happen in any bone in the body. The cause of chondroblastic osteosarcoma is unknown, but it has been linked to specific genetic mutations and environmental factors. It is most common in adolescents and young adults and is characterized by malignant cartilage-forming cells. The prognosis for chondroblastic osteosarcoma depends on several factors, including the size of the tumor and its location, how far it has spread, and the patient's age and general health. Treatment typically involves a combination of surgery, chemotherapy, and radiation. Here, we present a rare case of maxillary chondroblastic sarcoma in a 33-year old woman presenting with a mass in the right quadrant of the maxilla. The lesion is sized as 42*25*30mm and is expanded from the lateral incisor tooth region area to the tuberosity in the anteroposterior dimension, from the alveolar crest to the maxillary sinus.
| Published in | Science Futures (Volume 1, Issue 1) |
| DOI | 10.11648/j.scif.20250101.17 |
| Page(s) | 59-62 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Chondroblastic, Osteosarcoma, Case Report, Maxilla, Oral Cavity, Oral Pathology
CT Scans | Computerized Tomography Scan |
MRI | Magnetic Resonance Imaging |
CBCT | Cone Beam Computed Tomography |
OS | Osteosarcoma |
| [1] | Angiero, F., Moltrasio, F., Cattoretti, G., & Valente, M. G. Clinical and histopathological profile of primary or secondary osteosarcoma of the jaws. Anticancer Research. 2011; 31(12): 4485-4489. |
| [2] | Sasaki A, Miyashita H, Kawaida M, Kameyama K. Low-grade osteosarcoma is predominant in gnathic osteosarcomas: A report of seven cases of osteosarcoma of the jaw. Clin Exp Dent Res. 2021; 7(6): 1175-82. |
| [3] | Peddana, S. K., Ramadas, R., Cherian, E., & Thayalan, D. Chondroblastic and fibroblastic osteosarcoma of the jaws: Report of two cases and literature review. Indian journal of dental research: official publication of Indian Society for Dental Research. 2017; 28(1): 100-104. |
| [4] | Azizi T, Motamedi MH, Jafari SM. Gnathic osteosarcomas: a 10-year multi-center demographic study. Indian J Cancer 2009; 46: 231-3. |
| [5] | Taghavi N, Mehrdad L, Rajabi M, Akbarzadeh A. A 10-year retrospective study on malignant jaw tumors in Iran. J Craniofac Surg. 2010; 21: 1816-19. |
| [6] | Ketabchi A, Kalavrezos N, Newman L. Sarcomas of the head and neck: a 10-year retrospective of 25 patients to evaluate treatment modalities, function, and survival. Br J Oral Maxillofac Surg. 2011; 49: 116-20. |
| [7] | Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathologica. 2021; 113(2): 70-84. |
| [8] | Huh WW, Holsinger FC, Levy A, Palla SLF, Anderson PM. Osteosarcoma of the jaw in children and young adults. Head Neck. 2012; 34: 981-4. |
| [9] | Shirazian S, Agha-Hosseini F. Oral osteosarcoma: A case report and analysis of previously reported cases. N Y State Dent J. 2014; 80: 50-4. |
| [10] | Nissanka EH, Amaratunge EA, Tilakaratne WM. Clinicopathological analysis of osteosarcoma of jaw bones. Oral Dis. 2007; 13: 82-7. |
| [11] | Paparella ML, Olvi LG, Brandizzi D, Keszler A, Santini-Araujo E, Cabrini RL. Osteosarcoma of the jaw: An analysis of a series of 74 cases. Histopathology. 2013; 63: 551-7. |
| [12] | Neto P, Jean R, Tainah S, et al. CHondroblastic osteosarcoma of the maxiila: a case report. Oral Surg Med Pathol Radio. 2023; 136(1): 25. |
| [13] | Hasen Y M, Tawel H, Alreeshi K M, et al. Mandibular Chondroblastic Osteosarcoma: A Case Report. Cureus. 2024; 16(2): e53713. |
| [14] | Aymen Ben Fredj et al. Chondroblastic osteosarcoma of the distal tibia: a rare case report. Pan African Medical Journal. 2017; 27: 11. |
| [15] | N. Pai, G Menon, G Harshavardhan. Chondroblastic osteosarcoma – Does this rare histological variant warrant a change in management?: A case report. Journal of Orthopaedic Reports. 2022; 1(4). |
| [16] | Mamachan P, Dang V, Bharadwaj NS, DeSilva N, Kant P. Chondroblastic osteosarcoma-A case report and review of literature. Clin Case Rep. 2019 Sep 30; 8(11): 2097-2102. |
| [17] | N Bhardwaj, V Bachhal; U Nahar Saikia. Chondroblastic osteosarcoma. Autops Case Rep. 2023; 13: e2023466. |
APA Style
Mostafazadeh, S., Taeby, A., Abdal, F. (2025). Chondroblastic Osteosarcoma of the Maxilla: A Rare Case Report. Science Futures, 1(1), 59-62. https://doi.org/10.11648/j.scif.20250101.17
ACS Style
Mostafazadeh, S.; Taeby, A.; Abdal, F. Chondroblastic Osteosarcoma of the Maxilla: A Rare Case Report. Sci. Futures 2025, 1(1), 59-62. doi: 10.11648/j.scif.20250101.17
@article{10.11648/j.scif.20250101.17,
author = {Samira Mostafazadeh and Aria Taeby and Fariba Abdal},
title = {Chondroblastic Osteosarcoma of the Maxilla: A Rare Case Report},
journal = {Science Futures},
volume = {1},
number = {1},
pages = {59-62},
doi = {10.11648/j.scif.20250101.17},
url = {https://doi.org/10.11648/j.scif.20250101.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.scif.20250101.17},
abstract = {Osteosarcoma is a malignancy of mesenchymal cells that have the ability to produce osteoid or immature bone. Chondroblastic osteosarcoma as constitute a substantial proportion of all osteosarcomas of the jaws. Some examples may be composed almost entirely of malignant cartilage growing in lobules with only small foci of direct osteoid production by tumor cells being identified. Chondroblastic osteosarcoma is a rare and aggressive type of bone cancer that tends to occur in the long bones of the arms and legs, although it can happen in any bone in the body. The cause of chondroblastic osteosarcoma is unknown, but it has been linked to specific genetic mutations and environmental factors. It is most common in adolescents and young adults and is characterized by malignant cartilage-forming cells. The prognosis for chondroblastic osteosarcoma depends on several factors, including the size of the tumor and its location, how far it has spread, and the patient's age and general health. Treatment typically involves a combination of surgery, chemotherapy, and radiation. Here, we present a rare case of maxillary chondroblastic sarcoma in a 33-year old woman presenting with a mass in the right quadrant of the maxilla. The lesion is sized as 42*25*30mm and is expanded from the lateral incisor tooth region area to the tuberosity in the anteroposterior dimension, from the alveolar crest to the maxillary sinus.},
year = {2025}
}
TY - JOUR T1 - Chondroblastic Osteosarcoma of the Maxilla: A Rare Case Report AU - Samira Mostafazadeh AU - Aria Taeby AU - Fariba Abdal Y1 - 2025/12/09 PY - 2025 N1 - https://doi.org/10.11648/j.scif.20250101.17 DO - 10.11648/j.scif.20250101.17 T2 - Science Futures JF - Science Futures JO - Science Futures SP - 59 EP - 62 PB - Science Publishing Group SN - 3070-6289 UR - https://doi.org/10.11648/j.scif.20250101.17 AB - Osteosarcoma is a malignancy of mesenchymal cells that have the ability to produce osteoid or immature bone. Chondroblastic osteosarcoma as constitute a substantial proportion of all osteosarcomas of the jaws. Some examples may be composed almost entirely of malignant cartilage growing in lobules with only small foci of direct osteoid production by tumor cells being identified. Chondroblastic osteosarcoma is a rare and aggressive type of bone cancer that tends to occur in the long bones of the arms and legs, although it can happen in any bone in the body. The cause of chondroblastic osteosarcoma is unknown, but it has been linked to specific genetic mutations and environmental factors. It is most common in adolescents and young adults and is characterized by malignant cartilage-forming cells. The prognosis for chondroblastic osteosarcoma depends on several factors, including the size of the tumor and its location, how far it has spread, and the patient's age and general health. Treatment typically involves a combination of surgery, chemotherapy, and radiation. Here, we present a rare case of maxillary chondroblastic sarcoma in a 33-year old woman presenting with a mass in the right quadrant of the maxilla. The lesion is sized as 42*25*30mm and is expanded from the lateral incisor tooth region area to the tuberosity in the anteroposterior dimension, from the alveolar crest to the maxillary sinus. VL - 1 IS - 1 ER -
Department of Oral and Maxillofacial Pathology, Urmia University of Medical Sciences, Urmia, Iran
Faculty of Dentistry, Urmia University of Medical Sciences, Urmia, Iran
Department of Oral and Maxillofacial Pathology, University of Medical Sciences, Ilam, Iran